Resources & Insights
Expert articles on OCD, anxiety, and mental wellness — backed by research.
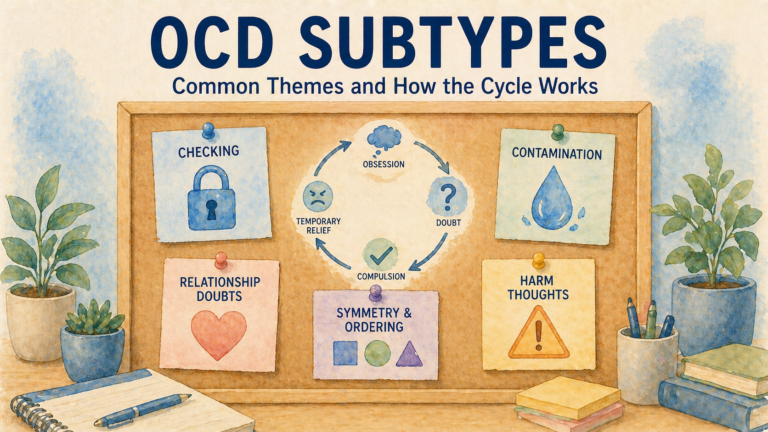
OCD Subtypes: Common Themes and How the Cycle Works
OCD subtypes describe common themes like contamination, harm, checking, and relationship doubts. Learn why the OCD cycle matters…
Read More →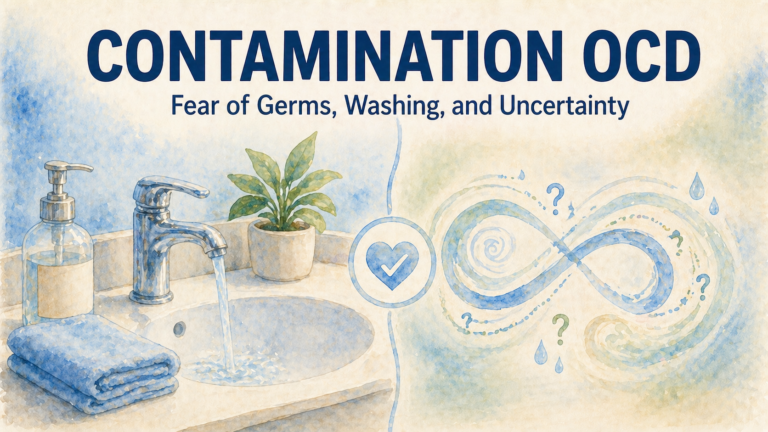
Contamination OCD: Fear of Germs, Washing, and Uncertainty
Contamination OCD can involve fear of germs, illness, chemicals, or feeling contaminated. Learn how the cycle works and…
Read More →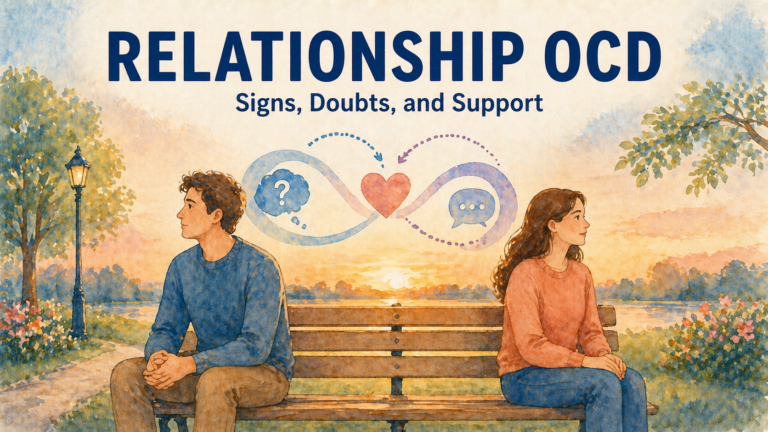
Relationship OCD: Signs, Doubts, and Support
Relationship OCD can involve repeated doubts, checking feelings, and reassurance seeking. Learn how ROCD works and what support…
Read More →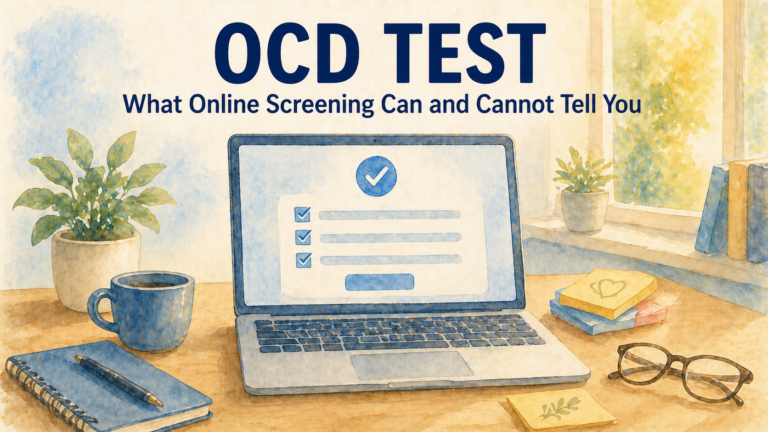
OCD Test: What Online Screening Can and Cannot Tell You
An OCD test can help you notice symptom patterns, but it cannot diagnose you. Learn what online OCD…
Read More →
OCD Therapy: What to Expect from ERP and CBT
Learn what OCD therapy may involve, including CBT, ERP, exposure planning, response prevention, progress tracking, and between-session practice.
Read More →
OCD Treatment Options: CBT, ERP, Medication, and Self-Help Support
Learn about common OCD treatment options, including CBT, ERP, medication, and self-help tools, plus when to seek professional…
Read More →
Intrusive Thoughts: What They Are and When They May Be OCD
Intrusive thoughts are unwanted thoughts, images, or urges. Learn when they may be part of OCD and what…
Read More →
Understanding Pediatric OCD and Anxiety: A Cognitive-Behavioral Approach to Family Resilience
Obsessive-Compulsive Disorder (OCD) in children presents unique challenges that can greatly affect their school performance and family dynamics.…
Read More →
Understanding Pregnancy and Postpartum OCD: A Cognitive-Behavioral Approach to Maternal Mental Wellbeing
Pregnancy and postpartum periods can be overwhelming, often exacerbating conditions like OCD. Many mothers face intrusive thoughts including…
Read More →Start Your Recovery Journey Today
Take the first step with evidence-based tools designed by clinical psychologists. Free for 7 days.
Get the App Free →